Quick version
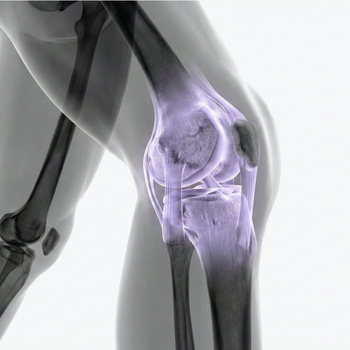
Three Common Knee Culprits: How They Differ
Having knee pain is a broad term. To understand your injury, we need to look at where it hurts and how the pain originated.
1. Meniscus Injuries: The Shock Absorber That Wears or Tears
Meniscus acts as the knee's shock absorber. Injuries here are often divided into two categories:
- The Acute Twist: Typical for sports like padel or football where the foot gets stuck in the surface while the body rotates. It often feels like a sharp stab and can be followed by the knee "locking."
- Degenerative Injury (Wear and Tear): For the experienced exerciser, the meniscus can become more brittle over the years. No specific trauma is needed here; a deep squat can be enough to cause a tear in the already worn tissue.
2. ACL Injury: When Stability Disappears
The anterior ACL (cruciate ligament) is crucial for the knee's stability forward and during rotation.
Symptoms: A "popping" sound is often heard at the moment of injury. Unlike meniscus injuries, the knee usually swells significantly within just an hour.
The Sensation: The most typical description is "giving way" – a feeling that the lower leg and thigh are not connected and that the knee buckles under load.
3. Runner's Knee: The Classic Overuse Injury
Here, it's not about something breaking, but about a tendon rubbing against bone.
Symptoms: A distinct, aching pain on the outside of the knee. It rarely appears immediately, but creeps up after a few kilometers on the running track or at the end of a session.
Cause: It is often due to a combination of weak hip muscles and increasing training intensity too quickly. It is rarely dangerous but requires patience and specific rehab rather than just rest.
"Good" vs. "Bad" Pain – Get to Know Your Body
It is a myth that all training should be painless, but it is crucial to know which pain you can work through.
Good Pain (Reactive Pain): A dull ache that arises during exercise but does not increase progressively and fades by the next day. This is often a sign that the tissue is being loaded and strengthened.
Bad Pain (Warning Pain):
- Stabbing Pain: Like a knife in the joint during specific movements (typical for the meniscus).
- Nocturnal Pain: If the knee aches while you are resting.
- Locking: If you cannot fully straighten or bend your leg.
- Severe Swelling: A sign of an ongoing inflammatory process or bleeding in the joint.
From Self-Diagnosis to Confirmed Diagnosis
When neither rest nor light rehab helps, it's time to find out what is actually happening under the skin. The path to the right treatment always begins with a professional assessment, and there are several paths to take:
- Physiotherapist (Physical Therapist): Often the best first step. A physiotherapist performs clinical tests (such as bending, angling, and loading the knee) to see how menisci and ligaments react. In many cases, they can provide a diagnosis directly through these manual tests without the need for X-rays.
- Doctor and Orthopedic Surgeon: If major structural damage is suspected, such as an ACL rupture or a locked meniscus, a doctor or orthopedist should be consulted. They can assess whether surgical intervention or more advanced pain relief is required.
- MRI Scan (MRI): This is the "gold standard" for seeing soft tissues like menisci, cartilage, and cruciate ligaments. An MRI provides an extremely detailed image and is often used before a potential decision on surgery or when the clinical picture is unclear.
- Arthroscopy (Keyhole Surgery): In some cases, this is used as both a diagnostic tool and treatment simultaneously. The surgeon enters with a camera to see exactly what the injury looks like and can often fix the problem at the same time.